acute bacterial sinusitis
- related: General
- tags: #note
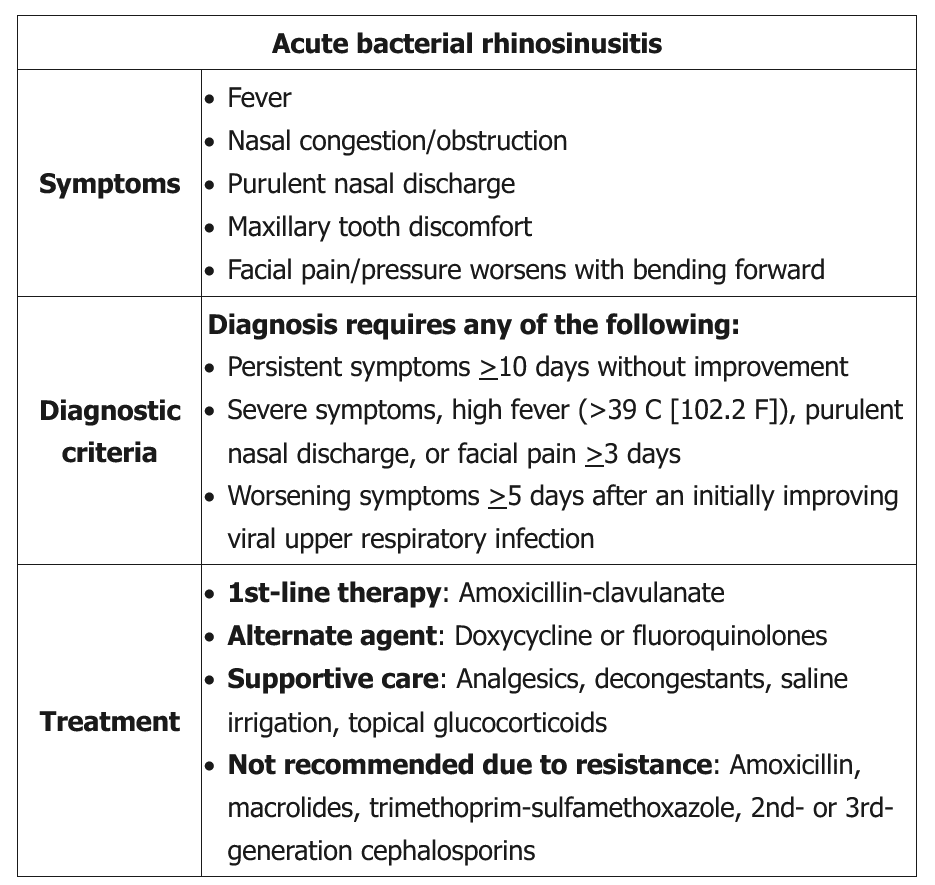
Most acute sinusitis seen in the primary care setting is viral in origin and is associated with the common cold. There is no evidence that antimicrobial treatment is effective in treating viral sinusitis. However, differentiating between viral and bacterial sinusitis is difficult. Acute bacterial sinusitis should be considered in patients with symptoms > 10 days; severe symptoms with fever > 39 C (102 F), purulent nasal discharge or facial pain > 3 days; or worsening symptoms > 5 days after an initially improving viral upper respiratory infection (Choice C).
Indications for antibiotic therapy for suspected rhinosinusitis
- Persistent symptoms lasting more than 10 days
- Severe symptoms, high fever (>39°C or 102°F), purulent nasal discharge or facial pain > 3 days
- Worsening symptoms > 5 days after an initially improving viral upper respiratory infection
Current guidelines recommend amoxicillin-clavulanate for 5-7 days to treat acute bacterial sinusitis in non-penicillin allergic patients. Amoxicillin is not the drug of choice due to increasing resistance of respiratory pathogens (e.g., Streptococcus pneumonia and Haemophilus influenza). Macrolides (e.g., azithromycin, clarithromycin), trimethoprim-sulfamethoxazole, and 2nd or 3rd generation cephalosporins are also not recommended as first-line agents due to increasing resistance involving the same respiratory pathogens. Doxycycline and respiratory quinolones (e.g., levofloxacin, moxifloxacin) are alternatives for penicillin-allergic patients. Quinolones or high-dose amoxicillin-clavulanate (2000 mg/125 mg) is recommended in patients who fail initial therapy.